


Author: Dr. Zhang, ZhangyeReproductive Medicine Research Institute,
Zhangye Reproductive Medicine SpecialHospital

Overview
Pulmonarynodules are a very common manifestation of chest imaging. Pulmonary nodules aresmall, local and round with an increased shadow density on the imaging. Theycan be single or multiple, without atelectasis, hilar enlargement or pleuraleffusion. Single pulmonary nodules do not have typical symptoms. They areusually shadows that cannot be penetrated by X-rays, single, clearly defined,denser, ≤30 mm in diameter and surrounded by air-permeable lung tissue. Locallesions > 30 mm in diameter are called lung masses.
Inrecent years, with the popularization of DR and CT equipment, especially thewidespread clinical use of dynamic DR, the number of pulmonary nodules foundduring chest examinations has increased significantly. The precise diagnosis ofsolitary pulmonary nodules has always been difficult in imaging diagnostics.This article focuses on the clinical application experiences of dynamic DR inthe diagnosis and diagnostics of pulmonary nodules in our hospital.
Key points of pulmonarynodule imaging analysis
Pulmonary nodules can be divided as multiple nodules and singlesolitary nodules. The clinical symptoms of most solitary nodules are notobvious, and they are often found during chest fluoroscopy in a physicalexamination. There is a good natural contrast in the chest, and X-ray examinationis an important means of finding and diagnosing pulmonary nodules. In thedifferential diagnosis of benign and malignant pulmonary nodules, combined withvarious signs of pulmonary nodule imaging and clinical data of patients, a moreaccurate diagnosis can often be made.
The discovery of pulmonary nodules should be comprehensivelyanalyzed from the location of nodules, the size of the nodules, the shape ofthe lesion, the density, cavities, and pleural changes, as well as hilar andmediastinal lymphadenopathy.
Location of pulmonarynodules
Size of pulmonarynodules
Diameter of ≤7 mm is defined as micronodules, diameter of 10 mmis defined as small nodules, diameter of 10-30 mm is defined as large nodulesand masses with a diameter of> 30 mm. The concept of nodules and massesshould be distinguished. Nodules and masses can be different developmentprocesses of the same disease. It has been reported in the literature that thesize of solitary pulmonary nodules has a certain qualitative significance,which is helpful to the identification of benign and malignant. Single pulmonarynodules with a diameter of less than 30 mm are mostly benign. The larger thediameter, the greater the probability of malignancy. Whether it is a benignnodule or a malignant nodule, the growth process is from small to large, so itis necessary to observe the dynamic changes of the lesion. Benign nodules are aslow-growing process, while malignant nodules mostly show progressive growth,mostly without calcification, and patients are mostly over 40 years old.Pulmonary nodules with a doubling time of 5-18 weeks are more malignant.
Shape ofLesion
Density of Lesion
The key to calcification in nodules depends on the shape anddistribution of calcification. Centrality, stratified, popcorn-likecalcification, or ring-shaped calcification are the characteristics of benigncalcification. For example, hamartomas can have popcorn-like calcifications,and tuberculous bulbs often have annular envelope calcifications; eccentric,amorphous calcifications, or sand Granular calcification is often malignantnodular calcification, and calcification can be seen in lung metastases ofdigestive tract tumors and osteosarcoma.
Cavitation signs and bronchial air signs are mainly found inlung cancer, more commonly in highly differentiated adenocarcinoma, and theirappearance or existence is of great value in the diagnosis of lung cancer.Benign tumors and inflammatory pseudotumor do not show this sign. This signshould be distinguished from fissure holes in the tuberculosis bulb.
Cavities can be seen invarious nodules. The cavities of lung cancer are characteristic: thick-walledeccentric (distal eccentric) cavities, and nodules are seen on the inner wall.The cavity of the tuberculosis bulb is mostly near the drainage bronchus, whichis an eccentric cavity at the proximal end. The cavity wall is thin and smooth.Tuberculosis lesions (satellite stoves) are common around the cavity. The cavitywall of the inflammatory pseudotumor is thick and the inner wall is smooth.Pulmonary metastases can have cavities. The inner walls of the cavities are smooth,and the walls can be uneven. Most of the cavity walls of Wegener’sgranulomatosis are thinner, and a few of them are thicker, but the edges of theouter wall are usually clearer, and there are no changes in leaves and burrs.The cavity can be reduced or disappeared after treatment.
Pleural Change
Application Advantagesof Dynamic DR
Multifunctional digital dynamic DR (dynamic DR) has been widelyused in clinical imaging diagnosis. Its multi-function, high-definitionimaging, real-time spot film, real-time playback, continuous spot film, wholebody stitching and other functions have been widely recognized for itsimportant role in clinical applications.
Case
This case is special because the right lower lobe nodular lesionis in the posterior Costco sacral region and is positioned lower back. Duringthe static DR chest PA examination, the nodular lesion is projected below thediaphragm, and the static DR cannot have visual image capture and rotatingfluoroscopy. No chest LAT were taken, plus the inexperience of the examiningdoctor, which led to misdiagnosis.
This case is enough to prove the importance of dynamic DR visualimage capture and the rotating multi-angle observation function in clinicalapplication, which can effectively avoid and reduce missed diagnosis andmisdiagnosis.

PA: The shadow of the right lungnodule is projected below the diaphragm(←)。

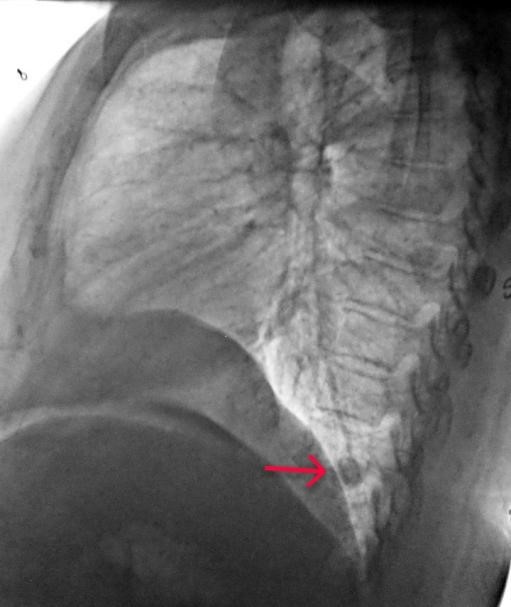
LAT: The nodular shadowis located in the posterior basal segment of the right lower lobe and theposterior costal corner(→)。

FluoroscopyFrame 1:Shadow position of right lung nodule during deep inspiration(←)

Fluoroscopy Frame 2:Shadowposition of right lung nodule during deep exhalation(←)
Fluoroscopy Frame 3: Lateral perspective observation of the rightlower inferior lobe nodule shadow located in the posterior costal corner region(→)
